
- Home
- Minimally Invasive Surgery
- Patient Education
- Enlarged Prostate / BPH
- Kidney Stones
- Urinary Incontinence
- Urinary Frequency
- Kidney Tumors
- Kidney Cancer Educational Websites
- Kidney Cancer
- Kidney Tumor Active Surveillance
- Laparoscopic Kidney Removal (Nephrectomy)
- Robotic Partial Nephrectomy
- CT-guided Radiofrequency Ablation of Kidney Tumors
- Laparoscopic Radiofrequency Ablation of Kidney Tumor
- Nephroureterectomy
- Laparoscopic & Robotic Nephroureterectomy
- Prostate Cancer
- Bladder Cancer
- Testicular Cancer
- Male Sexual Problems
- Urology News
- About
- Contact Us
 We have listed the accepted surgical treatment options for kidney stones. Selection of the "right" treatment depends to the location, type and size of stones as well as the understanding what each patient wants and tolerates. At times we combine several treatments to help render the patients "stone free."
We have listed the accepted surgical treatment options for kidney stones. Selection of the "right" treatment depends to the location, type and size of stones as well as the understanding what each patient wants and tolerates. At times we combine several treatments to help render the patients "stone free."
Shockwave Lithotripsy

ESWL Machine and Setup
Extracorporeal Shockwave Lithotripsy, “ESWL” for short, was developed in the 1980′s. It works by using sound waves to break kidney stones. It is the least invasive stone surgery.
What it involves?
Patients lay on their back on a special operating table. After sedation, an gel apparatus that looks like a giant breast implant (see second photo) is placed against the patient’s back side on the site where the kidney stone is present. Loud and powerful sound waves are then produced by various methods, depending on machine type.
We used to have patients inside a large pool of water, but switched to a more convenient gel-based media to transmit the sound waves.
The challenge then is to use the ESWL machine’s X-Rays to identify and target the sound waves onto the stone. On average, 2,000 shock waves are then delivered to the stone and “treatment success” during the operation is noted when a sharply denoted stone at the beginning of treatment on X-Ray is more “fuzzy” or hazy towards the end.

ESWL Treatment Head
Obviously, the hard part for some patient comes AFTER the treatment, when these fragments have to actually pass.
Thus, our clinical experience and research recommends this treatment to patients with smaller stones (<1cm) so that the fragments after ESWL would be small enough to pass easily.
In those patients who have larger stones or several stones that are targeted with ESWL, we typically recommend placing a stent (a plastic tube resembling a straw) to help prevent the kidney from becoming blocked while the stone fragments are passing down and out.
Placing a stent requires a urologist to look inside the bladder with a cystoscope (camera).
After treatment is complete, patients are awaken and taken to the recovery area. A couple of hours of observation are typical afterwards. Patients are expected to have pain that is normally eased with tablet pain medications.
This surgery is normally done in the outpatient setting and thus patients are sent home same day unless there are other health problems that require an admission to the hospital.
Length of Surgery
Typically less than one hour, but may be longer depending on how long it takes to sedate a patient, how well the stone is targeted and whether a stent needs to be placed. Like a lot of things in surgery, the actual treatment is quick, but the setup in the OR, patient positioning, sedation and preparation takes often more time than expected.Anesthesia
May be done with moderate sedation General anesthesia (heavy sedation with a ventilator) is recommended for best results. With general anesthesia, we are able to control patient's breathing and thus allow for better targeting of the stone.Benefits
- Least invasive kidney stone surgery
- Go home same day
- No skin incisions
- Works well with smaller stones
- Least painful in most cases
- Least potential damage to the urinary tract from instrumentation
Acute Risks
- <10% Risk of "Steinstrasse" (stone fragments scattered and blocking the tube that drains the kidney)
- <1% Severe urine infection requiring hospitalization
- Incomplete stone fragmentation
- Incomplete passage of stone fragments
- 5-30% Kidney bleeding (from mild bruising from small vessel to large vessel bleeding from the shockwave forces)
- Flank (back) pain
- Blood in the urine is very common and resolves within the first 24 hours
- <1% Risk of injury to organs next to the kidney (i.e. pancreas, intestines)
Chronic Risks
- Risk of developing high blood pressure (hypertension)
- Further stone production
- Patients with baseline renal dysfunction may be at risk for further renal damage from shockwaves
- Incomplete passage of stone fragments
- Kidney bleeding (bruising from small vessel or large vessel bleeding from the shockwave forces)
Ureteroscopy
The “ureter” is the natural, narrow tube that drains each kidney. This is the tube where kidney stones may try to pass through and get stuck, causing pain. In the past 20 years, with the introduction of fiberoptic technology, we have developed thin cameras that are able to be placed in the ureter.

Flexible Ureteroscope – Thin flexible camera used to see the stone fragments inside the ureter and kidney
We are able to see inside the ureter and perform various procedures including the use of a small laser fiber to break stones into small fragments. We also have tiny wire baskets that we can use to grab small pieces of stones and remove them outside the body.
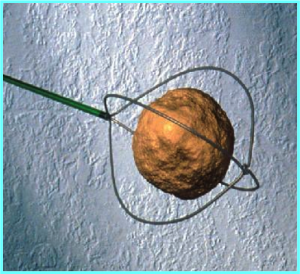
Stone captured in a small basket that is placed through the ureteroscope camera.
Almost all types of stones may be treated with ureteroscopy. Obviously, the larger the stone is, the longer it may take to break and remove each piece.
At the end of the procedure, most surgeons leave a stent (plastic tube) inside the ureter with a tip in the bladder. The stent is placed because the ureter gets swollen after instrumentation and the swelling may block the kidney after surgery (just like if you hit your finger, it gets swollen).
This surgery is normally done in the outpatient setting and thus patients are sent home same day unless there are other health problems that require an admission to the hospital.
What it involves?
After patients are asleep with general anesthesia, patients lay on their back in stirrups. The surgeon initially uses a small camera to look inside the bladder and place a small wire up to the kidney that has the kidney stone. Using the wire as our guide, surgeon places the thinner camera (ureteroscope) and may see the entire drainage tube (ureter) as well as the inside of the kidney.
Once the stone is identified, a special tiny laser fiber is used to crack the stone into very fine fragments which then are left to pass naturally or if large enough are then removed with tiny baskets that are placed through the camera.
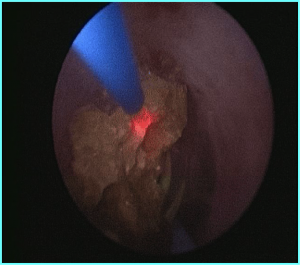
Lasering (laser fiber in blue) of a stone (yellow) done through the ureteroscope.
Length of Surgery
Ureteroscopy length of surgery primarily depends on the size of the stone. Most ureteroscopy procedures take about 1-2 hours to complete.Anesthesia
General anesthesia (heavy sedation with a ventilator) is recommended for best results. With general anesthesia, we are able to control patient's breathing and thus allow for better targeting of the stone as we use the laser to break the stone.Benefits
- Minimally-invasive approach
- Go home same day
- No skin incisions
- Works well with smaller stones
- Higher rate of complete stone clearance when compared to ESWL
- Lasers, unlike sound waves, are able to fragment almost every type of stone
Acute Risks
- Possible incomplete stone removal
- Urine infection requiring hospitalization
- Potential damage to the ureter or kidney
- Stent related pains, (bladder and/or kidney pains)
- Blood in the urine is very common and resolves within the first 24-48 hours, though as long as the stent is in place, some mild bleeding is very much expected
Chronic Risks
- Further stone production
- Potential for scar tissue development along the ureter that may produce obstruction of the kidney
Percutaneous Lithotripsy (PCNL)
Percutaneous (through the skin) lithotripsy refers to a treatment of kidney stones through a small cut in the skin made in a person’s back side, which is directly behind the kidney.
This approach allows for a surgeon to get access to the kidney directly from the skin without going through the bladder or ureter. The small stab incision is usually the size of a dime, but that is actually large enough to allow the use of our larger available instruments that can break the stone into pieces that may be removed from the kidney with ease.
This approach is ideal for patients with very large stones >2 cm (just under an inch and larger). Whereas ureteroscopy is limited by the use of very thin instruments, making the procedure time consuming, if we are treating a larger stone, percutaneous lithotripsy (PCNL) allows us to remove pieces as big as 1 cm with each pass of our instrument into the kidney. We also have very efficient and powerful tools besides the laser technology, such as the ultrasonic stone breakers and hammer-like pneumatic machines.
To learn more about the machines used you may see their websites:
1. ACMI/Olympus Cyberwand
2. Boston Scientific Lithoclast
3. Cook StoneBreaker
What it involves?
After patients are asleep with general anesthesia, patients typically have a small catheter placed the bladder. Then patients are positioned to lay on their belly with their back up. Next, using x-ray and/or ultrasound guidance and usually with the help of an x-ray doctor (radiologist) a needle is placed from the skin directly into the kidney with the stone. With the same incision, we are then able to dilate the tract, to create a tunnel from the skin directly into the kidney. Through this tunnel, we then are able to place a larger camera inside the kidney, visualize the stone and proceed with stone removal with graspers and are able to pulverize the stone into smaller pieces that are further removed.
At the conclusion of the procedure, and depending on the duration of surgery, presence of bleeding, we conclude the surgery by leaving a tube that sticks out from the incision in the back side of the patient. This drain is temporary and is usually removed once urine clears up from bleeding and there are no plans to look back into the kidney.
In rare cases, the volume of stones is so large, that I discuss with patients the possibility of doing at least 2 trips to the operating room to clear out all the stone burden because taking care of all stones in one trip to the operating room may just take too much time under anesthesia.
Length of Surgery
PCNL length of surgery primarily depends on the size and location of the stone. At times it is difficult to access the kidney from the skin and sometimes it is a struggle to get in the correct spot with our instruments to reach the stone. With stone burden 1-3 cm, the procedure usually lasts about 2 hours, however, with larger stone and those especially taking up a lot of the kidney, the procedure may take up to 3+ hours, though, in these cases, I often prefer to split the operation into 2 trips, so as to decrease side effects of prolonged anesthesia.Anesthesia
General anesthesia (heavy sedation with a ventilator) is recommended for best results. With general anesthesia, we are able to control patient's breathing and thus allow for better targeting of the stone and also control pain during the operation.Benefits
- Minimally-invasive approach, replaced the large incision open surgery for kidney stones
- Works very well for very large stones
- Higher rate of complete stone clearance when compared to ESWL and Ureteroscopy when it comes to stones > 2cm
- We are able to use multiple types of energy (ultrasonic waves, laser and pneumatic) to fragment almost every type of stone
Acute Risks
- Typically requires an overnight hospital stay
- Possible incomplete stone removal
- Urine infection requiring hospitalization
- Potential damage to the ureter or kidney
- Drain related back pain
- Blood in the urine is very common and resolves within the first 24-48 hours, though as long as the stent is in place, some mild bleeding is very much expected
- Since this procedure requires a puncture through the meat of the kidney, there is a risk of severe bleeding that rarely requires further procedures to stop bleeding and ever more rarely may result in severe damage or loss of the kidney
- Since the procedure requires a puncture through the skin and the kidney is located close to the lung, liver, spleen and bowel, rarely patients may suffer a collapsed lung or a puncture in the surrounding organs which requires an additional procedure(s) to correct the problem
Chronic Risks
- Further stone production
- Potential for scar tissue development in the kidney, though significant kidney damage has not been shown from the procedure, unless a patient required multiple punctures to clear the stone burden